
Published on October 28, 2020

Paula Andrea Forero
Radiology Research Assistant
Fundación Santa Fe de Bogotá

Ángela Moreno
Radiologist, Department of Cardiothoracic Imaging
Fundación Santa Fe de Bogotá

Bibiana Pinzón
Radiologist, Department of Cardiothoracic Imaging
Fundación Santa Fe de Bogotá
In March 2020, Colombia first faced what would become the cause of a new kind of chaos in this country: the coronavirus disease (COVID-19) pandemic. Nobody knew for sure what it was about, but one certainty was that we had to be prepared for the fight. However, it wasn’t as simple as it sounded, especially in a country were the health care system teeters every day on that fine line between sustainability and collapse.
In an undeveloped region, Colombia experiences barriers to health constantly. Despite having a policy that, ideally, aims to guarantee access and equity, the reality reveals the opposite. In this case, the COVID-19 outbreak tipped the balance further in favor of disparity: across the country, hospital infrastructure and capacities were not sufficient. Medicines—sedatives, anesthetics agents, even oxygen—and supplies, such as ventilators, were also in short supply. In addition, the availability of personal protective equipment (PPE) varied according to the prestige of the institutions; therefore, it was not uncommon to see health care workers in rural areas exposed to the virus without any protective measures. Not to mention that social indiscipline contributed to poor epidemiological control. With the arrival of the COVID-19 vaccine, things didn’t change much. Compared to countries on continents like North America and Europe, Colombia in northern South America has a very low rate of vaccination. Only 16.5% of Colombians are vaccinated. Vaccine prioritization is determined by the government, depending upon age and the availability of boosters, which are scare at times.
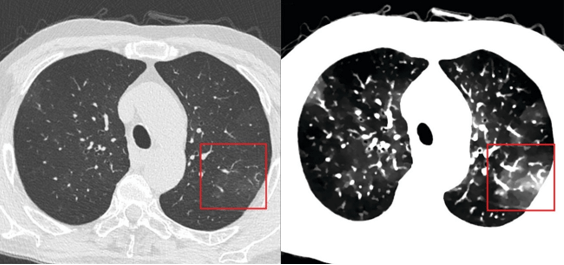
As our lives changed, so did our work in medicine. Undoubtedly, medical imaging and diagnostic radiologists became even more important resources in this battle. The demand for our specialty increased enormously, bringing new challenges to overcome. Radiologists had to learn a new language—the language of COVID-19—which included new imaging classifications, findings, and approaches (Fig. 1).
The radiological diagnosis of a new, lethal entity was in our hands. Regarding personnel, technicians, nurses, and radiologists remain on the front lines, due to their contact with ill or potentially infected patients; and as for statistics, the number of chest radiographs and CT scans increased exponentially throughout this period. They are still our most requested studies.
However, these numbers have been very fluctuant. At the beginning of the pandemic, in March and April of 2020, when both quarantine and curfew were established, the number of imaging studies related to COVID-19 at our institution in Bogotá were 77 and 160, respectively. Come August, our total COVID-19-related images numbered 1,617, coinciding with the country’s epidemiological peak. This year, January, May, and June have been the months with the most imaging evaluations made (1,953, 2,823, and 3,124, respectively), surpassing what we interpreted in many months of 2020. These data show that as the virus evolved and infection control and prevention became more lax, Colombians forgot about self-care and contagion increased significantly, producing an evident strain on medical staff and the entire health care system.
This situation is not over yet. Although many advances have been made, there is still a lot of uncertainty—still a long way to go. Hopefully, better days are coming for Colombia and for all of us. COVID-19, beyond doubt, represents a lesson to countries around the world in reassuring the public health care system as a fundamental pillar of society.
The opinions expressed in InPractice magazine are those of the author(s); they do not necessarily reflect the viewpoint or position of the editors, reviewers, or publisher.