
Updated October 25, 2021

Jonathan R. Dillman
Associate Chief of Research, Department of Radiology
Cincinnati Children’s Hospital Medical Center
@therealjonadill
AJR Pediatric Imaging Section Editor
2021 ARRS Symposium Course Codirector
Practical Pediatric Imaging

Rama S. Ayyala
Associate Professor of Radiology
Cincinnati Children’s Hospital Medical Center
@rayyalamd
2021 ARRS Symposium Course Codirector
Practical Pediatric Imaging
Practical pediatric imaging education, especially virtually, benefits most from a combination of didactic lectures and interactive case-based reviews that are relevant for a broad audience: dedicated pediatric radiologists, general radiologists who interpret pediatric imaging examinations, and radiology trainees—residents and fellows.
On September 8 and 9, the ARRS Virtual Symposium, Practical Pediatric Imaging, provided a head-to-toe review of both standard and novel, state-of-the-art methods, delivered by an esteemed and diverse faculty. If you were not able to attend this live symposium, the following offers a perfect primer.

Practical Pediatric Imaging Online Course
Reviewing a range of pediatric abnormalities—including neonatal and neuroimaging, as well as musculoskeletal and body disorders—this Online Course also discusses imaging appropriateness and key features of both conventional and emerging methods.
During the neonatal session, Judy H. Squires of UPMC Children’s Hospital in Pittsburgh addressed neonatal head ultrasound, including the application of newer imaging methods, such as ultrasound elastography and contrast-enhanced ultrasound (Fig. 1).
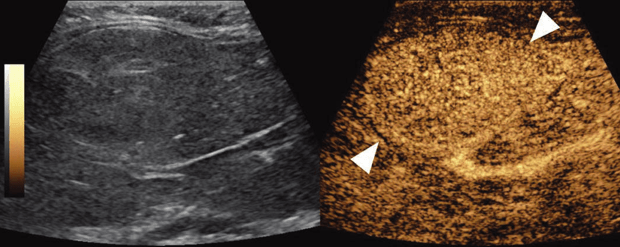
Recently, AJR published Squires’ “Contrast-Enhanced Ultrasound in Children: Implementation and Key Diagnostic Applications” manuscript. According to her review, “contrast-enhanced ultrasound utilization is rapidly expanding, particularly in children, for whom there is a growing range of FDA-approved and off-label diagnostic indications throughout the body.” Noting that ultrasound contrast agents lack renal excretion and can be administered to neonates, Squires concluded that the research thus far points to an “excellent pediatric safety profile of ultrasound contrast agents.” Squires’ facility with contrast-enhanced ultrasound implementation, as well as her knowledge of the supporting evidence in children, proved to be prized assets. Likewise, ARRS Symposia course codirector Rama S. Ayyala’s update on evaluating the vomiting infant was a boon for the curriculum, as was the comprehensive review of neonatal chest disorders from Peter J. Strouse of C. S. Mott Children’s Hospital in Ann Arbor, MI.
After Nancy A. Chauvin of Penn State Health Children’s Hospital in Hershey expertly examined pediatric arthritis, bone tumors, and bone marrow disorders, Strouse, senior author of the recent AJR Expert Panel Narrative Review on “Debunking Fringe Beliefs in Child Abuse Imaging,” explained how misattributing injuries leaves children at risk for future abuse (Fig. 2).
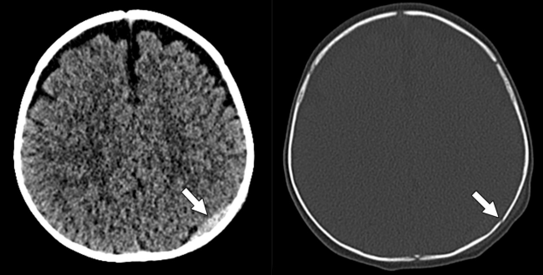
“Careful review of the scientific evidence and professional society consensus statements is important in differentiating findings attributable to child abuse from fringe beliefs used to discount the possibility that a child’s constellation of injuries is consistent with abuse,” Strouse maintained. He then listed the three categories that these fringe beliefs most often fall into:
- legitimate alternative diagnoses that should be considered;
- real disorders with actual findings that do not mimic child abuse;
- fabricated pathologies.
Meanwhile, 2018 ARRS Scholar Rupa Radhakrishnan of the Riley Hospital for Children at Indiana University Health in Indianapolis led an enlightening session on contemporary imaging and pediatric stroke, later helping ARRS Symposia course codirector Jonathan R. Dillman and Andrew T. Trout, also of Cincinnati Children’s Hospital Medical Center, to steer the interactive case-based review session. Additional neuroimaging lectures were given by Children’s Healthcare of Atlanta researcher Neil Lall, who skillfully detailed congenital brain malformations and pediatric brain tumors.
Following the thorough analyses of pediatric renal and liver tumors by Ayyala and Squires, respectively, Trout shared his multimodality assessment of adrenal tumors—staging, treatment response, the role of nuclear medicine—with Dillman joining to discuss peritoneal, mesenteric, and omental disorders, as well as congestive hepatopathy and Fontan-associated liver disease. (Fig. 3). For more Trout and Dillman research, turn to page 16 for a summary of their study on reduced-dose CT for lung nodules in children and young adults with cancer.

Trout was the primary author, alongside Ayyala and Squires, on yet another AJR Expert Panel Narrative Review, “Current State of Imaging of Pediatric Pancreatitis”. Imaging timing, secretin-enhanced MRCP, urgent MRI, severity prediction, autoimmune pancreatitis, serial imaging best practices—these are all distinct concerns for imaging pediatric acute, acute recurrent, and chronic pancreatitis. Trout and colleagues’ appraisal concluded with a 12-point consensus statement and structured reporting template; we are still studying both. Apropos, AJR editor in chief Andrew B. Rosenkrantz handpicked this Expert Panel Narrative Review to lead ARRS’ newest newsletter for in-training radiologists, The Resident Roentgen File.
The opinions expressed in InPractice magazine are those of the author(s); they do not necessarily reflect the viewpoint or position of the editors, reviewers, or publisher.