
Published March 1, 2022

Jasmine Gandhi
Department of Radiology
Beth Israel Deaconess Medical Center

Jordana Phillips
Department of Radiology
Boston Medical Center
Contrast-enhanced mammography (CEM), also known as contrast-enhanced spectral mammography and contrast-enhanced digital mammography, is a diagnostic imaging modality approved by the US FDA in 2011. With this technique, information regarding physiologic enhancement is obtained in conjunction with density and morphologic information obtained from digital mammography.
CEM Basics
CEM begins with IV administration of nonionic iodinated contrast material at a dose of 1.5 mL/kg and rate of 3 mL/s. Acquisition of CEM images begins 2 minutes after the start of the injection. To perform CEM, the standard four views of a mammogram (craniocaudal and mediolateral oblique of each breast) are acquired by means of dual-energy technique, whereby low-energy images (below the K-edge of iodine) and high-energy images (above the K-edge of iodine) are performed for every imaging position. Although contrast material has already been administered, the low-energy images do not display contrast enhancement, and these images look like standard 2D mammograms. Studies have shown that low-energy images are not inferior to 2D images [1]. The high-energy images capture contrast material within the breast but are not directly interpretable. The mammography unit postprocesses the low-energy and the high-energy images to create a recombined set of images that are akin to subtraction images in breast MRI, which reveal areas of increased vascularity. The recombined images, which highlight contrast enhancement, are interpreted in conjunction with the low-energy images, which display the standard mammographic features of breast abnormalities. There is no current standard order of image acquisition, and imaging centers vary in their approaches.
Any additional diagnostic views to be obtained with dual-energy technique, such as spot compression and lateral views, typically are acquired after the standard four projections. All images must be acquired 2–10 minutes after contrast material injection to ensure adequate opacification of any abnormality.
A CEM report includes interpretation of both the low-energy images and the recombined images. As of this writing, there is no dedicated lexicon for CEM [2]. For this reason, low-energy images are currently described with BI-RADS mammography descriptors. Recombined images are described with BI-RADS MRI descriptors. Should either low-energy images or recombined images show suspicious features, further evaluation with diagnostic imaging or biopsy is needed. If the low-energy images reveal a concerning imaging finding, the finding should be worked up regardless of the presence or absence of enhancement, given that some cancers can, albeit infrequently, present without enhancement.
CEM has been studied primarily in the diagnostic setting, where it has been compared with mammography, mammography combined with ultrasound, and breast MRI. Overall, the performance metrics of CEM have consistently been found better than those of standard imaging with mammography and ultrasound with improved cancer detection and a higher NPV [3–7]. CEM has been found consistently to have a cancer detection rate similar to that of breast MRI with fewer false-positive findings [8–10].
CEM Advantages
The main advantage of CEM is that it provides standard mammographic information, while also providing physiologic information without the need for breast MRI. However, there are multiple other advantages of CEM.
First, there are fewer equipment, space, and personnel requirements. To perform CEM, some of the commonly used standard mammography equipment can be upgraded to allow dual-energy imaging. This includes the addition of a copper filter and software and firmware upgrades. As a result, practices across the country could begin using CEM without needing to purchase a new machine or acquiring more clinical space. In addition, mammography technologists can be trained to perform CEM, owing to its similarity to standard mammography, so no new personnel are needed.
Second, interpretation of low-energy images is like that of standard digital 2D mammograms, and interpretation of recombined images is like that of MRI subtraction images, sequences familiar to radiologists. As a result, learning to interpret CEM images is more achievable than learning an entirely new imaging technique.
Third, although CEM still involves radiation, the radiation does is well within the acceptable range for mammography [1, 2].
Last, CEM can serve as an alternative modality to breast MRI at medical centers where MRI may not be available or for patients with contraindications to MRI. The advantages of CEM compared with MRI are that it is a shorter examination, is less expensive, is more accessible, and has rates of diagnostic accuracy similar to those of MRI [1]. Moreover, patients tend to prefer CEM to MRI for screening and diagnostic imaging.
CEM Challenges
CEM is not without its challenges. The main challenge of CEM relates to contrast administration. There is the small but real risk of a contrast material–related event, such as contrast reaction, contrast extravasation, or contrast-induced acute kidney injury (CI-AKI). Severe contrast reactions, which include both allergy-like and physiologic reactions, have been reported at a frequency of 0.04% [11]. Fatal reactions are rare; the American College of Radiology contrast material manual [11] reports a frequency of fatal reaction among 170,000 patients. Those with prior reactions to contrast material or a history of atopy in general (e.g., asthma, urticaria) are at increased risk of development of a contrast reaction. Before receiving contrast material, patients must be assessed for contrast reaction risk factors. In addition, patients need to stay in the department for 15–30 minutes after CEM is performed to ensure that a reaction does not occur.
CI-AKI is acute renal injury caused by contrast material that develops within 48 hours of contrast administration. Recent data [11] suggest that CI-AKI is essentially nonexistent among patients with an estimated glomerular filtrate rate (eGFR) of 45 mL/min/1.73 m2 or greater and rare (0–2%) among patients with an eGFR of 30–44 mL/min/1.73 m2. As a result, some institutions have adopted a more relaxed approach to contrast administration and do not routinely measure eGFR, unless the patient has history of kidney disease or risk factors for kidney disease (such as diabetes or medically treated hypertension). Other institutions continue with a more conservative approach and measure eGFR for all patients and limit contrast use on the basis of the eGFR calculations.
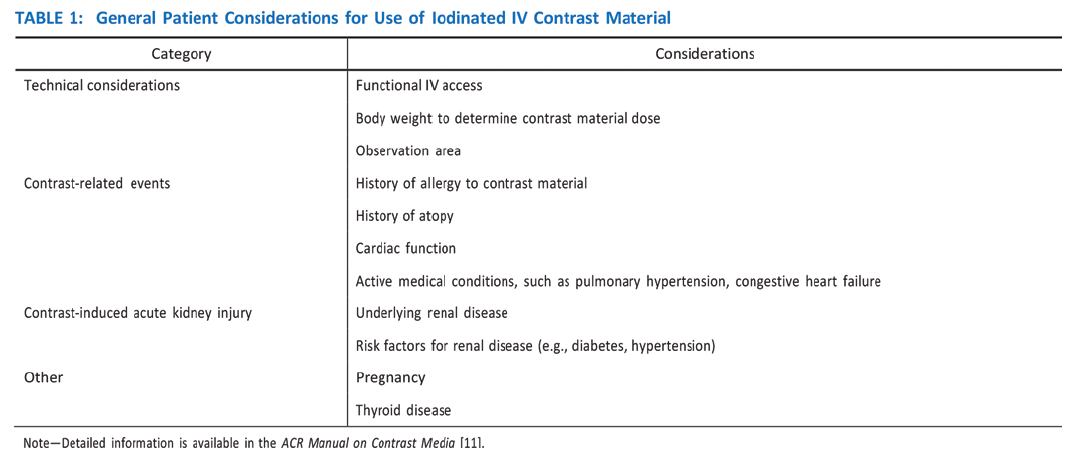
The safety assessments and care to minimize contrast-related events invariably prolong the patient’s time in the imaging department. There is the additional logistical challenge of finding time, room, and personnel for insertion of the IV line (Table 1).
Additional challenges of CEM relate to the risk of false-positive and false-negative results. For example, fibroadenoma, pseudoangiomatous stromal hyperplasia, abscesses, and papillomas are known benign entities that may exhibit contrast enhancement. Unfortunately, it is often not possible to prospectively determine that these imaging findings are benign, and biopsy is frequently necessary. False-negative findings can be caused by limitations of the imaging modality in capturing abnormalities along the chest wall, sternum, and axilla. Moreover, the natural tendency of the breast tissue to become enhanced (background parenchymal enhancement) can limit the ability to detect abnormal enhancement related to cancer. CEM artifacts, such as scatter radiation in the breast (matrix artifact or rim artifact), can also limit the ability to detect abnormal enhancement.
Last, CEM biopsy capability has been approved but is not universally available. As a result, when suspicious lesions are identified on recombined images only, further evaluation with standard digital mammography, ultrasound, or MRI is required for tissue sampling. This can lead to more patient imaging, which has the potential to increase patient costs and anxiety.
Current Applications
As of this writing, CEM has been approved by the FDA only as a diagnostic examination. For this reason, imaging practices are primarily using CEM as an alternative to MRI, when MRI cannot be performed. CEM is also used as a problem-solving tool in cases of known or suspected lesions. It is used in cases of recalls from screening; breast cancer staging (Fig. 1); evaluation of symptomatic breasts; troubleshooting complicated mammographic and ultrasound imaging, although this is rare; and treatment response to neoadjuvant chemotherapy. Some institutions are using CEM for supplemental breast cancer screening of patients who cannot undergo MRI, have dense breast tissue, or need additional screening.

Future Directions
Although screening mammography is associated with reduced mortality rates, it consistently underperforms in the evaluation of patients at high risk of breast cancer and those with dense breast tissue. Even with the addition of digital breast tomosynthesis, supplemental imaging with ultrasound and MRI is often recommended for these patients to improve cancer detection. However, ultrasound and MRI have their own sets of challenges. Ultrasound is operator dependent, time-consuming, and has a high false-positive rate. Similarly, MRI is time-consuming, has a high false-positive rate, is expensive, and is not readily available worldwide.
CEM has the unique advantage of functioning at the level of MRI without the associated limitations. For this reason, there is interest in using CEM for breast cancer screening, particularly in the subset of women at intermediate and increased risk of breast cancer. A few studies of CEM for screening have been conducted. One [12] showed improved performance of CEM compared with mammography; CEM showed an additional 13.1 breast cancers per 1,000 women screened. Pilot studies comparing CEM with breast MRI [9, 10] also had promising results. Moving forward, the multisite prospective Contrast-Enhanced Mammography Imaging Screening Trial will compare CEM with tomosynthesis for breast cancer screening. Additional areas of interest include improved understanding of the value of CEM for diagnosis. A study comparing the accuracy, feasibility, and cost of CEM compared with standard diagnostic imaging workup of patients recalled from breast cancer screening is currently underway. [5]. Other research is being conducted in areas of contrast-enhanced tomosynthesis, radiomics and artificial intelligence, and whether the CEM enhancement pattern can be predictive of cancer subtypes and treatment success.
A multimodality review—everything from routine ultrasound and mammography to the latest DBT and AI applications—ARRS’ Breast Tumor Imaging Online Course delivers the interpretive, technical, and systems knowledge that practicing radiologists need to provide quality breast cancer screening. Additional lectures address pathology, the BI-RADS lexicon, and even the history and economics of breast cancer, all critical for improving overall care disparities and patient outcomes.
Read faculty excerpts from the abbreviated breast MRI sessions on InPractice.
The opinions expressed in InPractice magazine are those of the author(s); they do not necessarily reflect the viewpoint or position of the editors, reviewers, or publisher.