
Published October 4, 2022

Richard Wiggins, MD
@RHWiggins
Associate Dean of CME
Professor of Radiology and Imaging Sciences
University of Utah Health Science Center
Subdivided at the hyoid bone, the soft-tissue core of the extracranial segment of the head and neck can be divided further into two discrete areas: the suprahyoid neck and the infrahyoid neck. Whereas the infrahyoid portion lies inferiorly between the hyoid bone and clavicles, the suprahyoid area comprises the deep spaces between the base of the skull and the hyoid bone. While decades ago, lesions in the deep suprahyoid neck lead to a vague report listing a long differential diagnosis, an understanding of the suprahyoid neck anatomic space can lead to an accurate space-specific differential diagnosis. Here, three layers of cervical fascia help to define all the separate spaces in the deep part of our face.
Presented live on Sunday, April 16 during the 2023 ARRS Annual Meeting in Honolulu, HI, our “The Suprahyoid Neck—Pathology Through Anatomy” Featured Session will focus on reviewing important anatomical subunits and common pathologies of the suprahyoid neck: the parapharyngeal, pharyngeal mucosal, masticator, parotid, carotid, retropharyngeal, danger, and perivertebral spaces (Fig. 1).
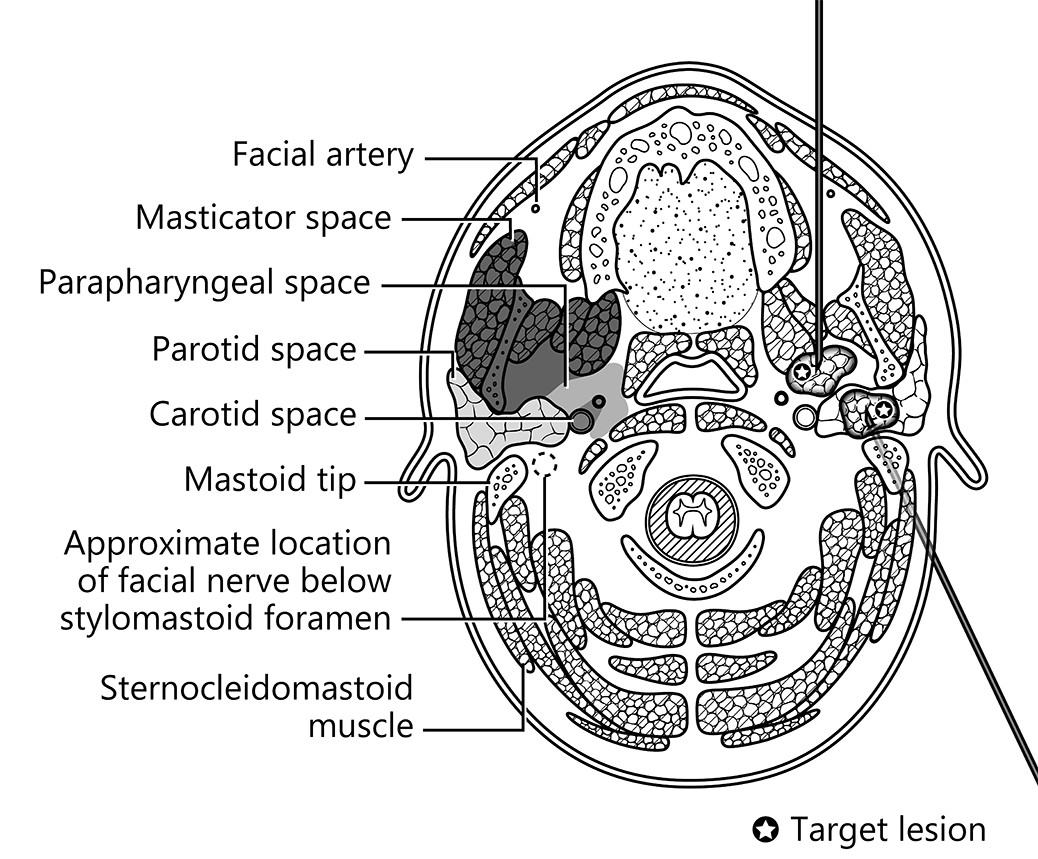
Examining imaging findings crucial for diagnostic radiologists and neuroradiologists alike to identify, attendees will enhance their clinical performance through a greater, more holistic understanding of cross-sectional anatomy and common pathologies that lead to various lesions in these regions—each a critical check point for accurate interpretation of radiological studies of the suprahyoid neck.
Speaking of studies, our illustrious Featured Sunday Session faculty are especially looking forward to leading breakout sessions regarding the various modalities most frequently found in imaging the suprahyoid neck. The comparative insensitivity of CT for artifacts, CT’s more comprehensive delineation of facial structures, and the promise of contrast-enhanced images to reveal critical vasculature continue to make CT more advantageous than ultrasound guidance (Fig. 2).


And because CT-guided fine-needle aspiration and biopsy can be performed with patients in three positions (supine, prone, lateral decubitus), multiple clinical studies in the imaging literature continue to conclude that this procedure remains safe and effective for obtaining tissue to diagnosis lesions of the head and neck. For quick reference, we encourage you to consult the following preprocedural patient care checklist for fine-needle aspiration and/or biopsy to help promote a professional and efficient imaging encounter with your patients:
- Procedure
- Relevant to ongoing care?
- Anesthesia
- Moderate sedation available?
- General anesthesia more appropriate?
- Consent Approval
- Both procedure and sedation?
- Imaging
- Preprocedural images available for review?
- Positioning
- Planned trajectory verified?
- Patient able to tolerate?
- Lab Results
- Values within acceptable ranges?
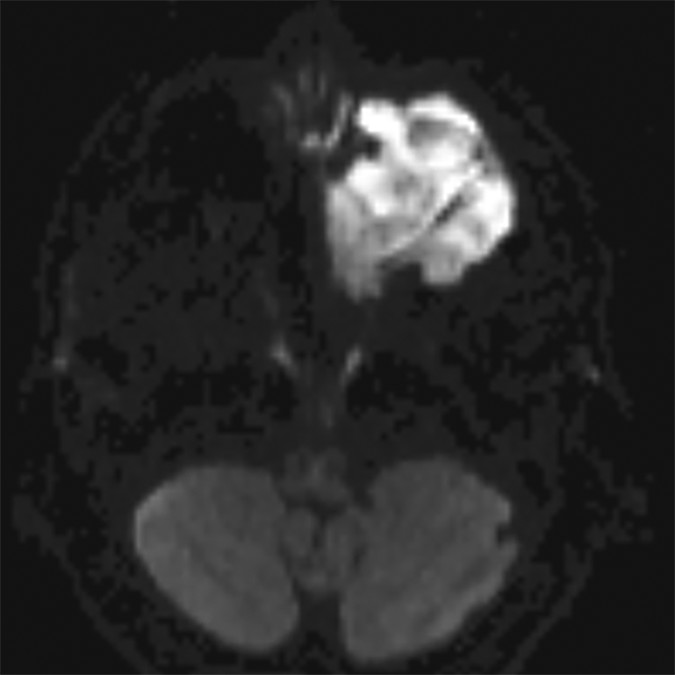
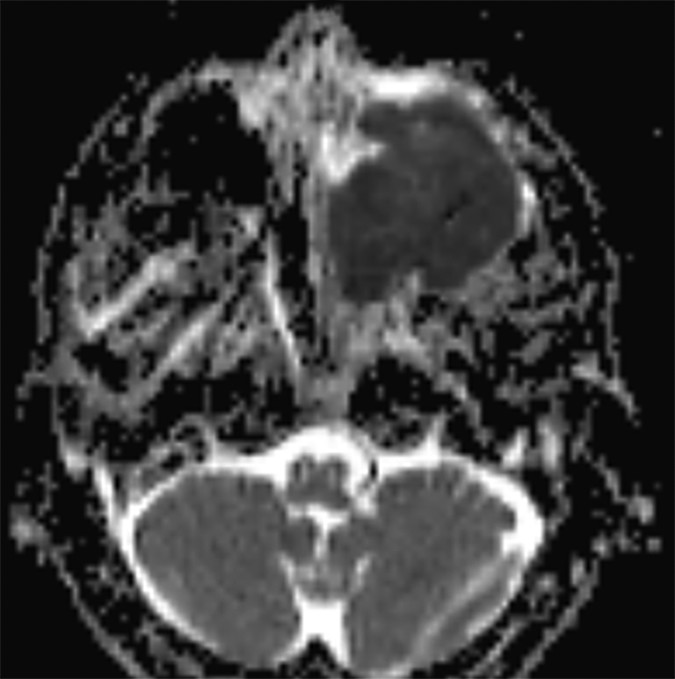
In certain instances, diffusion pulse sequences can offer a complementary adjunct to conventional MR pulse sequences, but neither diffusion-weighted imaging (DWI) or diffusion tensor imaging (DTI) should be utilized as a standalone technique for characterizing the benignity of head and neck lesions. Moreover, since mean apparent diffusion coefficients (ADC) values derived from DTI parameters are characteristically lower than ADC values developed from DWI parameters—frequently lower than reported malignant threshold values—the two should not be used interchangeably (Fig. 3).
With personalized, precision medicine becoming increasingly more critical for our patients in today’s value-based health care environment, the topic of the suprahyoid neck is particularly timely for medical imagers at all professional levels and of every practice type, notably so for head and neck radiologists, neuroradiologists, and in-training imagers of both subspecialties. Closely working alongside head and neck surgical teams—often on complex cases of deep space neck masses with widely differential diagnoses—practicing radiologists must intimately understand each significant space of the suprahyoid neck, as well as their surrounding fascial boundaries.
Unique in the quality of the educators and the breadth of the curriculum, our “The Suprahyoid Neck—Pathology Through Anatomy” live event from Oahu Island on Sunday the 16th will also address key concepts for radiologists to improve their accuracy in reporting complex imaging cases. A key didactic point will be how a better understanding of suprahyoid neck anatomy can lead the imager to a space-specific differential and diagnosis. Once again, just as we concluded the ARRS “Temporal Bone Imaging Made Easy” symposium this March, I will then review top points from all the earlier expert presentations. We will officially adjourn after another spirited Q&A block, allowing faculty to address individual questions regarding both anatomical and pathological considerations when imaging the suprahyoid neck spaces.
The Upper Aerodigestive Tract
Also presented live on Sunday, April 16 during the 2023 ARRS Annual Meeting in Hawaii, our “The Upper Aerodigestive Tract” session will review essential anatomy and pathology of this tract surrounding the suprahyoid neck spaces. Each subunit of the upper aerodigestive tract will be examined, including the nasal cavity, nasopharynx, oral cavity, oropharynx, larynx, hypopharynx, cervical trachea, and cervical esophagus. Esteemed faculty for this Featured Sunday Session have prepared clinically focused sessions on important anatomical subunits, examining cross-sectional anatomy and pathology findings that are critical for the head and neck radiologist to understand for each region. Participants will enhance their performance by gaining a greater understanding of common pathologies that occur, honing in on critical check points for accurate interpretation of head and neck imaging studies of the upper aerodigestive tract, which is critical for certain pathologies—especially so for squamous cell carcinoma.
As an instructional topic for medical imaging professionals, the upper aerodigestive tract is timely in today’s health care environment, too. Awareness and appreciation of the many issues that can arise are indispensable to rendering better health care for our patients. Specifically, when collaborating with head and neck surgeons on non-cutaneous head and neck squamous cell carcinoma cases, it is the imaging that determines the staging—and, therefore, the therapy—in these complex cases.
Similar to our “The Suprahyoid Neck—Pathology Through Anatomy” course on the same day, an overall primer on critical spaces will be presented first, before diving into the more detailed subunit lectures our experts have prepared. Once more, each region of the upper aerodigestive tract will be assessed in functional terms alongside normal imaging findings, followed by a thorough analysis of pathologies for common head and neck cancers, as well as important mimics and differentials.
The opinions expressed in InPractice magazine are those of the author(s); they do not necessarily reflect the viewpoint or position of the editors, reviewers, or publisher.